


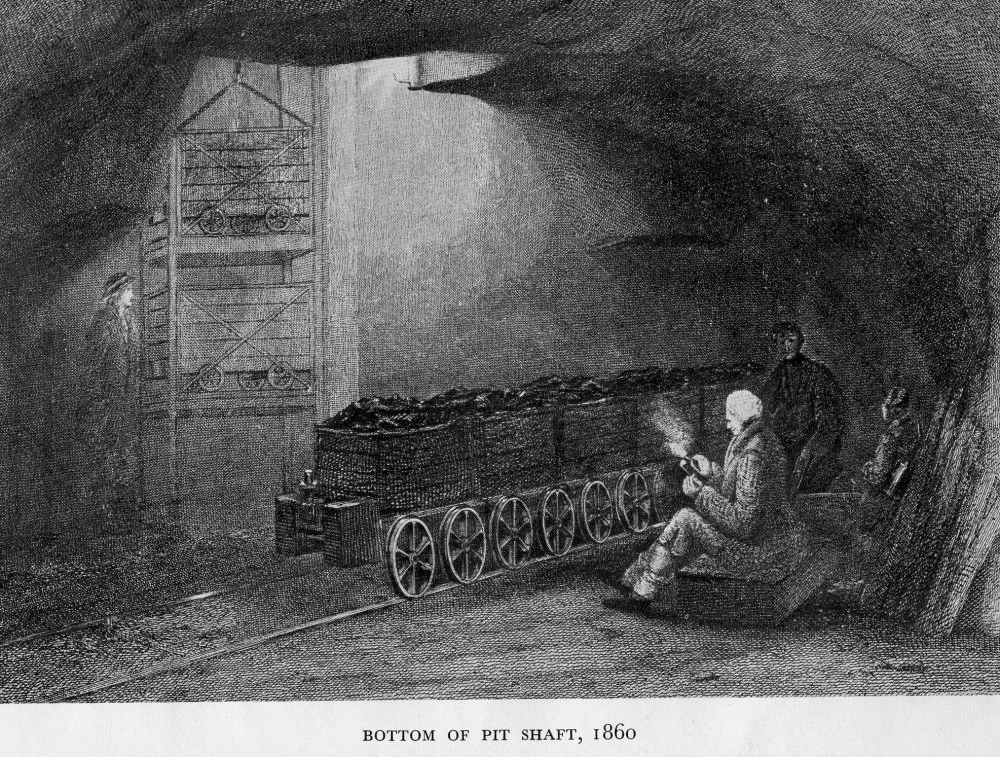
Photo Credit: Appalachian VoicesBlack lung disease is not new. Mining coal as a heating source goes back centuries, as does exposure to coal dust. It was this initial exposure that led to the first diagnoses of what would later be understood as “coal workers pneumoconiosis” (CWP), or black lung.
Coal’s usage for industrial purposes throughout the Industrial Revolution increased its global importance. Bituminous coal production in the US rose from around 20 million tons in 1860 to 243 million by the end of the century. Following the end of World War I, domestic coal production reached a peak at 527 million, declining sharply during the Great Depression to around 350 million in 1932, but reaching new heights of 620 million tons during World War II. King Coal’s legacy was cemented here, as were the prolific company towns, anti-union campaigns, worker uprisings and strikes, and a new market for coal’s usage.
However, CWP did not formally receive a medically-defined diagnosis until 1942 by the British Medical Research Council and it wasn’t until 1969 that coal miners and their dependents could first access federal disability benefits via the Federal Coal Mine Health and Safety Act.
The struggle to win medical and disability benefits is one that is deeply tied with the vested interests of corporations and politicians who refused to budge until the pressure of everyday advocates became too great to withstand. Below is an abridged timeline of relevant events detailing this struggle.
1831
Dr. James Gregory of Edinburgh, Scotland identifies dark pigment disorders in a patient, John Hogg, during his autopsy. Hogg was a coal miner who had been admitted to an infirmary complaining of breathlessness, chest pains, and severe coughs. Dr. Gregory’s medical notes highlight the contemporary medical issues with CWP. Dr. Gregory became the first medical doctor to argue that the conditions of coal miners and the inhalation of coal dust led to a patient’s death. His “Case of Peculiar Black Infiltration of the Whole Lungs, Resembling Melanosis” was the first report tying respiratory illness with an individual’s occupation as a coal miner.

1870s
Ohio Governor Rutherford B. Hayes established a Mining Commission to examine the conditions in the state’s coal industry. Dr. Daniel Rathben appeared before the commission in 1871 to give testimony on the respiratory ailments encountered in his coal-digging patients that were sometimes referred to as “spurious melanosis” or “coal miner’s consumption”. The physician noted that dust exposure brought on “a good many cases of Asthma.”
Rathben’s testimony led to the appointment of the state’s first mine safety officer. In 1889, he argued that there needed to be the establishment of a state hospital to accommodate victims of dust disease.

1900s
Miners’ asthma or anthracosis was widely recognized in biomedical circles, and clinicians had identified many of its signs and symptoms, but the cause of the disease remained uncertain in the community; with some physicians solely blaming exposure to dust, and others uncertain if the disease predated mining.
1930s
Built between 1930-1932, the Hawks Nest Tunnel served to divert water from the New River through Gauley Mountain to a hydroelectric plant, providing power for an electro-metallurgical plant in Alloy. The three-mile tunnel was constructed to move water to Union Carbide’s operations and employed hundreds of mostly Black migrant workers primarily from the US South. However, the speed at which workers were expected to construct this tunnel caused them to face incredibly high levels of silica dust exposure without any protective equipment, leading to the fastest and deadliest outbreak of acute silicosis in the nation’s history.
These Black miners faced brutal conditions, working longer shifts, being denied rest breaks in clean air environments, receiving payment in company scrip, and even reportedly being forced to work at gunpoint. As miners became too sick to continue, sheriffs would act as company enforcers and would force them out of the area leaving many to die in makeshift camps nearby.
The full scale of this tragedy only came to light during a 1936 Congressional hearing on the matter, where survivors would later testify about the horrific conditions they were exposed to. The House committee concluded that the Hawks Nest Tunnel was completed with “grave and inhuman disregard for all consideration for the health, lives, and future of the employees.” While Congress took no action against the companies themselves, the national outrage helped to spur the first National Silicosis Conference, convened by Secretary of Labor Frances Perkins, and led to the 1936 law requiring respirator use in dusty conditions, as well as broad recognition of silicosis as an occupational disease eligible for workers’ compensation.
Nearly 800 of the over 1,000 workers died from silicosis, many within a few months of exposure, with Black miners buried in unmarked graves on a nearby farm because they were prohibited from being buried in “white” cemeteries.

1968-69
On the morning of November 20, 1968, a thunderous blast echoed across Marion County, WV. Flames shooting upwards of 150 feet in the air signaled another mine explosion. The Farmington Mine Disaster that trapped ninety-nine miners and killed seventy-eight was one of the worst such mining disasters in the nation’s history.
Both West Virginia Governor Hulett C. Smith and Assistant Secretary of the Interior Jay Cordell provided rather blasé statements following the disaster. Governor Smith said, “We must recognize that this is a hazardous business, and what has occurred here is one of the hazards of being a miner,” while Secretary Cordell stated, “The company here has done all in its power to make this a safe mine.” They hadn’t.
It wasn’t until 1990 that MSHA would conclude their investigation into the disaster, finding that ventilation “was inadequate overall, and most probably non-existent in some areas.” A safety alarm that would trigger ventilation from methane buildup had been disabled by the mine’s chief electrician, while the fans which would usually kick on in such an event were unable to start due to this loss in signal.
The disaster itself catalyzed the formation of the Black Lung Association and the Miners for Democracy movement, a reform movement within the UMWA, by exposing the coal industry’s and the union’s neglect of miners’ health and safety. West Virginia coal miners, aided by doctors I.E. Buff and Donald Rasmussen, organized the Black Lung Association the following month with a demand for the state to recognize and provide compensation for coal workers’ pneumoconiosis.
In February of 1969, over 40,000 miners across the state went on a wildcat strike and gathered to protest at the Capitol. The strike forced the state to pass a strong black lung compensation law that year. This victory propelled national action, leading to the landmark Federal Coal Mine Health and Safety Act (1969), which established the first federal mandatory dust limits and a federal benefits program for miners disabled by black lung and their widows. The continued advocacy would later lead to the Black Lung Benefits Act of 1972, which opened up eligibility requirements for miners and survivors to receive these benefits.
1869
Dr. John Carpenter of Pottsville, Pennsylvania provides a report to the county medical society about occupational health and respiratory problems among anthracite coal miners. Dr. Carpenter likewise concludes that the inhalation of coal dust and other gases inside coal mines was “the most serious” source of occupational disease nationwide. In his cautionary advice to insurance companies, Dr. Carpenter stated, “I could not conscientiously advise any life insurance company to do business among miners, except on short periods of risk, and at large increase of percentage.”

1881
Dr. H. A. Lemen, President of the Colorado State Medical Society, presented a paper at the society’s annual meeting about his patient James McKeever, a miner of 30 years, who presented with a “harassing cough,” and coughed up more than a pint of black liquid a day. The report was written by the physician with the black substance, an action that had an evident impact and reflected the growing curiosity among Colorado physicians in the 1880s about the health consequences of coal mining.
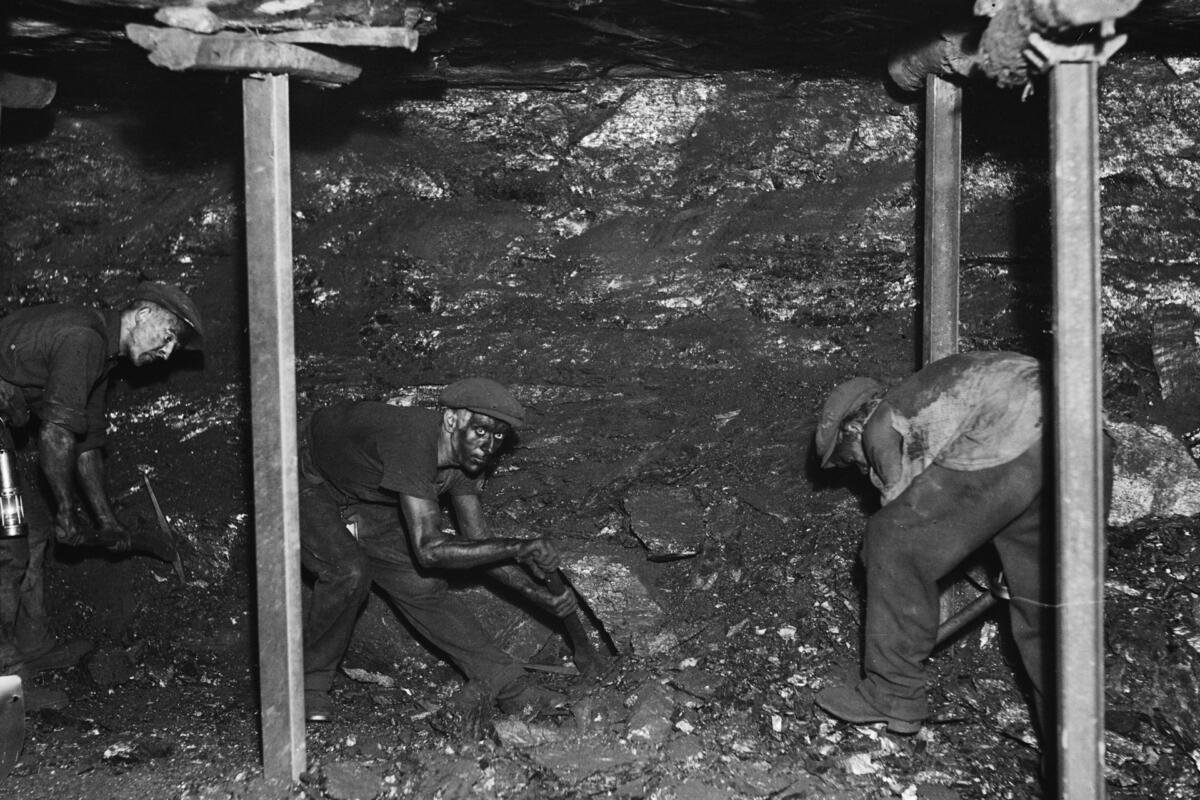
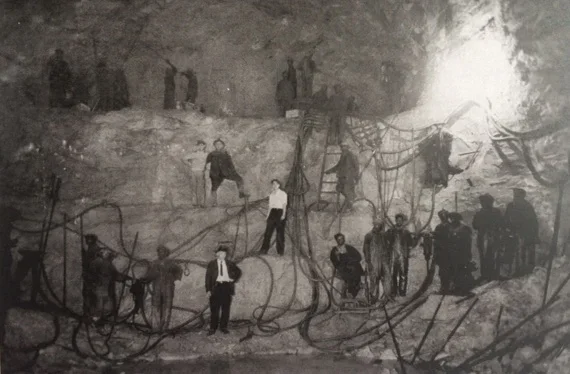
Photo Credit: Elkem Metals Collection, WV State Archives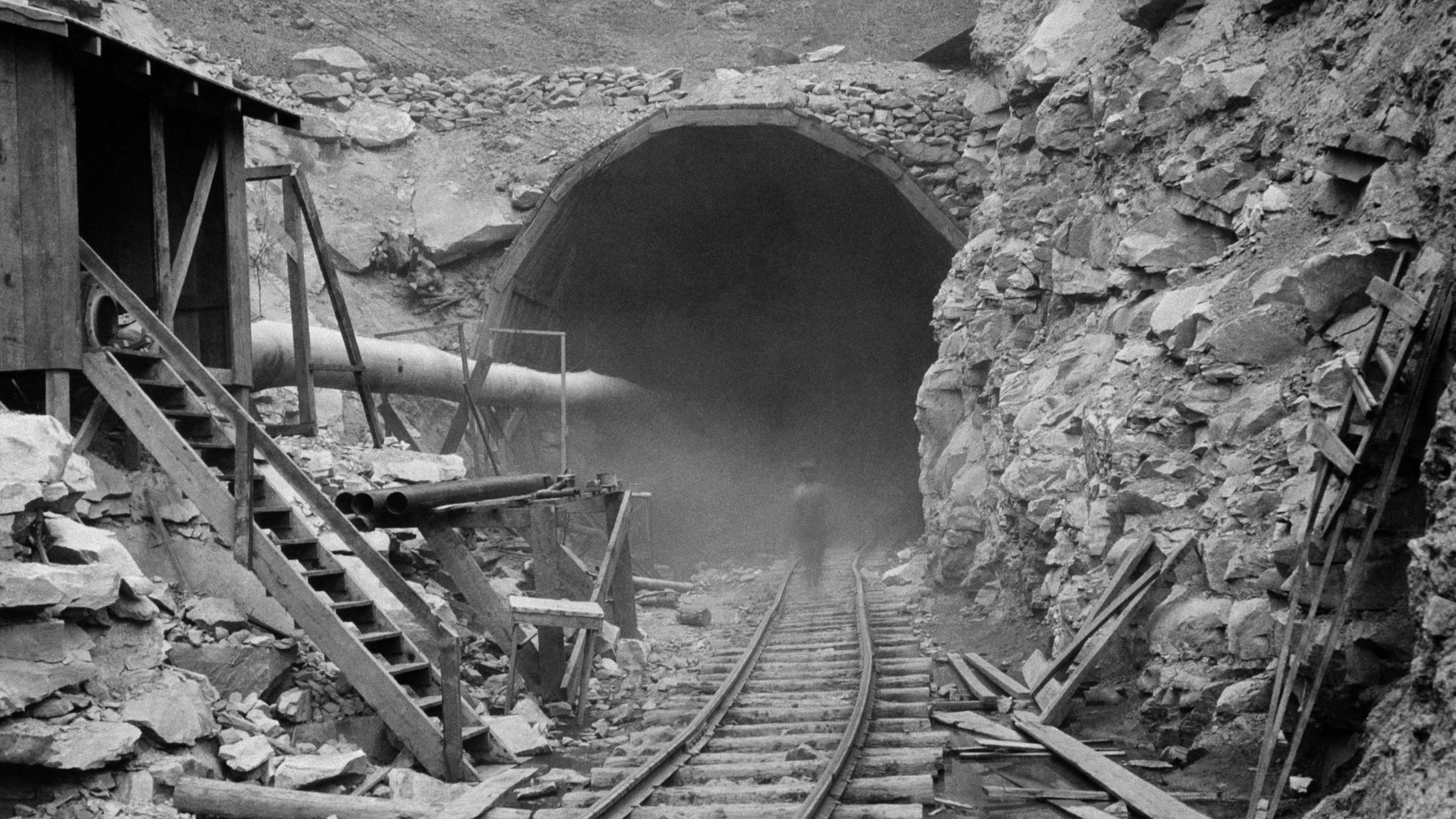
Photo Credit: Elkem Metals Collection, WV State Archives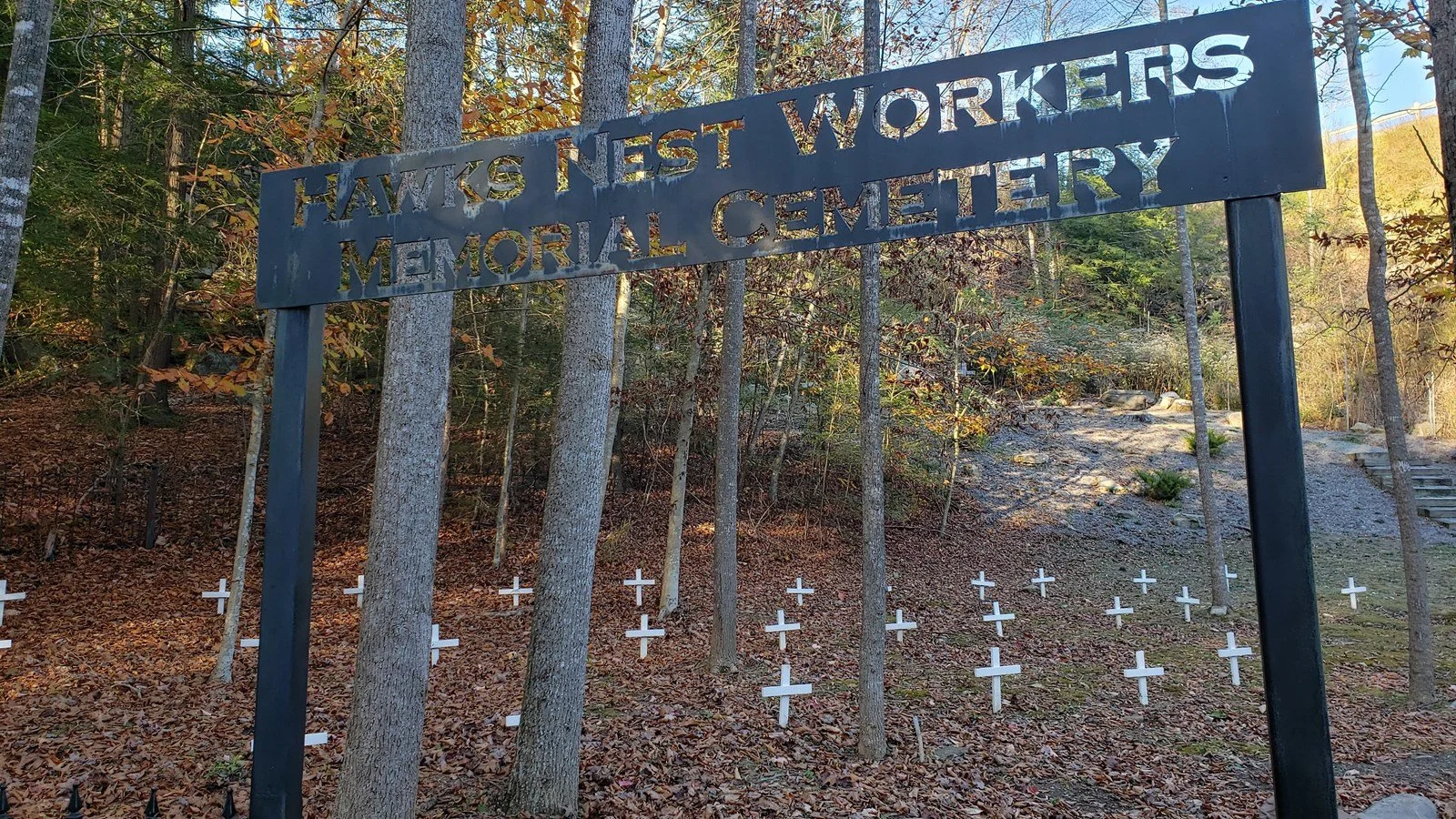
Photo Credit: NPS/Dave Bieri1950s
Following the end of World War II, the UMWA signed the National Bituminous Coal Wage Agreement with the Bituminous Coal Operators Association. Also known as the Mechanization Agreement, this contract authorized a massive extension in the mechanization process of unionized coal mines. While an increase in mechanization would lead to fewer employees per mine, the argument at the time was that it would reduce the laborious nature of coal mining, protect miners’ physical health, and increase wages as productivity rose.
Between 1950 and 1959, the number of coal miners nationwide dropped from 416,000 to 180,000. Those that remained employed faced increased, industrial-scale exposure to coal and silica dust.

Photo Credit: Mine Safety and Health Administration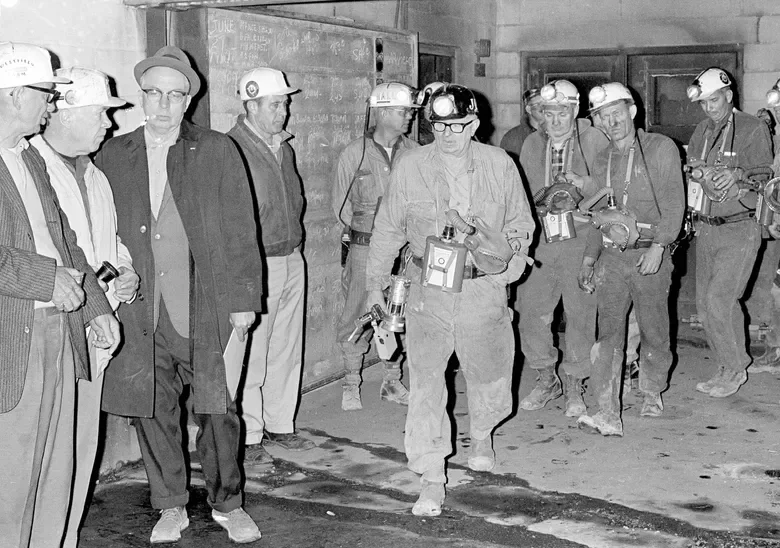
Photo Credit: AP Photo/File
Photo Credit: Earl Dotter1969
The Federal Coal Mine Health and Safety Act is a landmark piece of legislation that fundamentally reformed working conditions in US coal mines. Driven by the urgent need to address catastrophic incidents - such as the Farmington Mine Disaster - as well as the acute health issues of black lung disease, Congress responded with a package of legislation that is still in use today.
The opening to the Act remains relevant today: “The first priority and concern of all in the coal mining industry must be the health and safety of its most precious resource - the miner.” In response to the grassroots activism that followed the Farming Mine Disaster, the Act established the first federal mandatory coal dust limits to prevent higher exposure rates and required operators to strictly control respirable coal dust through engineering and administrative controls, with penalties for non-compliance.
Perhaps most crucially, Title IV of the Act created the first-ever federal black lung disability benefits program for miners totally disabled by black lung and their widows, funded initially by general tax revenue and established presumption linked to at least ten years of underground mine work to ease the burden of proof on claimants. The Coal Act also mandated that operators provide periodic chest X-rays of active miners to detect the disease early on and offer them the right to transfer to less dusty work areas if black lung was diagnosed.

1977
The Black Lung Benefits Revenue Act established a dedicated Black Lung Disability Trust Fund, financed by a new excise tax on coal, in order to pay benefits to miners whose former employers were no longer in business or could not be held liable for the disease. Its core significance was in shifting the financial burden of black lung compensation from the federal government and back to the coal industry while ensuring that there was a reliable, self-sustaining source of funds for miners. This legislation created a mechanism to hold mine operators accountable for long-term health liabilities, marking a critical first step in securing compensation for those disabled by black lung.

1991
At the turn of the decade, an MSHA employee noticed visible filter damage on a sample cassette, signaling that the operator-provided dust sample was likely fraudulent. After a 20-month investigation known as the “Great Coal Dust Scam,” the U.S. Department of Labor found that over 500 coal companies had systematically tampered with respirable dust samples intended to measure miners’ exposure to health hazards. Tampering methods at the time included vacuuming dust from pre-weighted filter cassettes, blowing dust out of samples, taking samples from outside of mines rather than inside work areas, and submitting inaccurate documentation intended to make dangerous working conditions appear compliant with federal regulations. By April 1991, Secretary of Labor Lynn Martin announced that MSHA had issued nearly 5,000 citations to companies in 847 mines and 504 operators across 16 different states. In total this was about 40 percent of active mines at the time. Proposed penalties totaled $5 million, the largest aggregate fine in MSHA’s history up to that time.
Some companies attempted to clear their name, claiming that inaccurate samples could be the result of outside forces rather than intentional attempts to game the system. Secretary Martin, for her part, condemned the widespread practice as “almost an addiction to cheat,” emphasizing that elevated dust levels going undetected posed severe health consequences for miners dying from black lung at a rate of nearly 4,000 annually. “What we do have,” Secretary Martin stated, “is evidence of a widespread attitude of indifference to miners’ health that allowed this kind of tampering with dust samples to take place.”
The scandal prompted immediate reforms, including requirements for tamper-resistance cassettes, the formation of an agency task force to improve the dust sampling program, and calls from labor advocates to transfer sampling responsibility from operators to government agencies with miners given oversight rights.
Photo Credit: CNN
Photo Credit: Ted Latusek2000-2014
Dr. Paul Wheeler was a radiologist at Johns Hopkins University Hospital who led their chest X-ray program for coal miners. The legal case against Dr. Wheeler centers around allegations that he intentionally failed to diagnose black lung disease among coal miners while he was working for various coal operators. This led to hundreds of wrongful denial of benefits for miners across the Appalachian coalfields. A Pulitzer Prize-winning investigation by the Center for Public Integrity in 2013 revealed that, from 2000 to 2012, Dr. Wheeler reviewed X-rays in more than 1,500 cases, interpreted over 3,400 films, and yet never once diagnosed a severe case of complicated black lung; this, even despite other doctors finding evidence of the disease in hundreds of the same cases.
Investigators documented at least 280 instances where Wheeler’s negative readings convinced administrative law judges to deny benefits, though later autopsies would prove that the miners did indeed have advanced black lung. Dr. Wheeler admitted in interviews that he had intentionally disregarded the International Labor Organization’s classification system required for federal black lung claims, stating that, “I don’t care about the law,” and that he had his own criteria for what constituted the disease.
Following the investigation, the Department of Labor issued a bulletin in June 2014, instructing officials to presume that Dr. Wheeler’s readings were not credible and not to credit his negative interpretations unless coal companies could provide persuasive evidence to rehabilitate his opinions. The Department of Labor also notified over a thousand miners that their claims may have been wrongfully denied and encouraged them to reapply. Johns Hopkins University suspended and later permanently discontinued its black lung program in 2015.
The saga of Dr. Wheeler highlights the recurring realities that, despite decades of laws, procedures, and regulations intended to decrease dust exposure and eradicate black lung, the disease persists as miners and their families continue to be denied benefits rightly owed to them. A system that is reliant on company experts, weak enforcement mechanisms, and legal immunity for biased testimony will continue to allow corporate interests to override medical evidence. In their wake are more dead miners, family members whose illnesses could have been prevented.

Photo Credit: WYMT
2011-2024
After the Upper Big Branch disaster, there have been significant strides made through federal regulatory actions to combat black lung disease, which have been subsequently followed by administrative rollbacks, legislative hurdles, and court challenges. The ebb and flow of this decade and a half coincided with significant drop off of mining employment in the Appalachian coalfields, the shuttering of coal-fired power plants nationwide, and the changing economic nature of Central Appalachia following the 2008 Recession.
During President Obama’s first administration, the Affordable Care Act included two crucial provisions of the Black Lung Benefits Act that had been eliminated in 1981. First, it reinstated the 15-year presumption, making it easier for miners with 15 or more years of work and a totally-disabling respiratory condition to qualify for benefits. Second, it restored automatic benefits for survivors of miners who were already receiving benefits at the time of their death, even if the death wasn’t directly caused by black lung.
A year before the Upper Big Branch Mine Disaster, MSHA launched its “End Black Lung - Act Now!” campaign. The agency-led campaign’s primary goal was to overhaul an outdated oversight program that had failed to protect miners from the disease. The result was a push for new, stricter regulations on respirable coal dust, culminating in their 2014 coal dust rule. The overall dust standard was lowered from 2.0 to 1.5 milligrams per cubic meter of air, real-time dust monitoring with continuous sampling to allow for immediate corrective action, and mandating sampling for a miner’s full shift under more representative working conditions.
The campaign is considered a success insofar as national average respirable coal dust concentrations reached a new low with high industry compliance rates. Moreover, MSHA reported that 2016 was the safest year in domestic mining history, with the lowest number of mining deaths annually ever recorded up to that point.
However, these positive regulatory changes were later rolled back during the first Trump administration. In 2017, MSHA initiated a regulatory review of the 2014 coal dust rule, seeking to make it “less burdensome” on operators. This created uncertainty about the future of dust exposure protections at the time, although MSHA would not implement the proposed regulatory changes. Additionally, in 2019, the Black Lung Disability Trust Fund’s main source of revenue - the domestic coal excise tax - was cut in half, from $1.10 and $0.55 per ton for underground- and surface-mined coal respectively to $0.50 and $0.25 per ton. Effectively, this change significantly increased the Fund’s overall debt, with estimates by the Governmental Accountability Office (GAO) anticipating that the Fund’s outstanding debt could exceed $15 billion by 2050.
Under the Biden Administration, two important regulatory changes took place supporting coal miners. First was the final silica dust rule, issued in April 2024, which lowered the permissible exposure limit for respirable crystalline silica to 50 micrograms per cubic meter, cutting the previous limit in half and finally aligning miners’ protections with those in other US industries. It also established an action level of 25 micrograms per cubic meter, requiring monitoring and added medical surveillance requirements, and established the primacy of engineering rather than administrative controls to protect miners.
At the end of his term, the Biden Administration also finalized their coal operator self-insurance rule, effectively closing the loophole that exists allowing coal operators to shift nearly $1 billion in black lung liabilities onto taxpayers. The new rule requires self-insured coal operators to set aside 100% of their black lung benefit liabilities as collateral, ending a practice whereby companies backed only about 19% of their obligations before declaring bankruptcy and dumping this cost onto the already-strained Black Lung Disability Trust Fund.

Photo Credit: West Virginia Public Broadcasting
Photo Credit: Earl Dotter1972
The Black Lung Benefits Act (1972) significantly expanded the original 1969 program by liberalizing eligibility requirements to make it easier for miners with black lung and their families to receive benefits. The Act extended coverage to orphans of black lung victims, adding approximately 2,000 children to benefits, while broadening the definition of the term “miner” to encompass both underground and surface miners. When President Nixon signed the bill into law, he acknowledged that the Act was a significant departure from state-run workers’ compensation processes given that so many coal-producing states had failed to adequately address the crisis of black lung disease’s rise.

1981
The Black Lung Benefits Amendments of 1981 was the beginning of restrictive measures intended to limit eligibility for benefits and reduce medical presumptions that had previously favored miners and their survivors. Its core significance was to tighten the criteria for black lung compensation, effectively shifting the burden of proof back onto miners and widows while doubling the excise tax on coal to address the Black Lung Disability Trust Fund’s then-growing deficit. These changes included the elimination of certain presumptions and stricter survivor benefits, such as requiring widows to prove that the miner’s death was due to CWP directly.
Photo Credit: Rockford Register Star
Late 1990s-Early 2000s
Between 1970 and the mid-1990s, black lung disease prevalence among tenured miners plummeted from nearly 35% to less than 5%. The most severe form of black lung disease, Progressive Massive Fibrosis (PMF), reached historic lows in the 1990s when only 31 unique cases were identified by the national surveillance program during the entire decade. Advanced black lung disease was so rarely detected that public health officials viewed this decline as a genuine triumph. Many assumed that existing cases were likely caused by exposures that occurred prior to the 1969 Coal Act and that, within a few years, no further cases would be detected.
However, the government’s optimism was not without caution. As early as 1995, Secretary of Labor Robert Reich would acknowledge that, despite significant progress, “the most recent medical evidence indicates that miners continue to be at risk of developing occupational lung disease.” Secretary Reich established an advisory committee to make recommendations “for the elimination of pneumoconiosis among coal miners” later that year. NIOSH had also issued a draft document in 1993, concluding that the risk of developing black lung at the current dust standard of 2.0 milligrams per cubic meter of air was greater than was previously predicted.
These concerns would later prove prescient. Beginning in the early 2000s, surveillance data began to show a strong and ongoing resurgence of the disease, particularly among Central Appalachian coal miners, where the prevalence of PMF eventually became higher than when NIOSH started to formally track the disease in the 1970s.
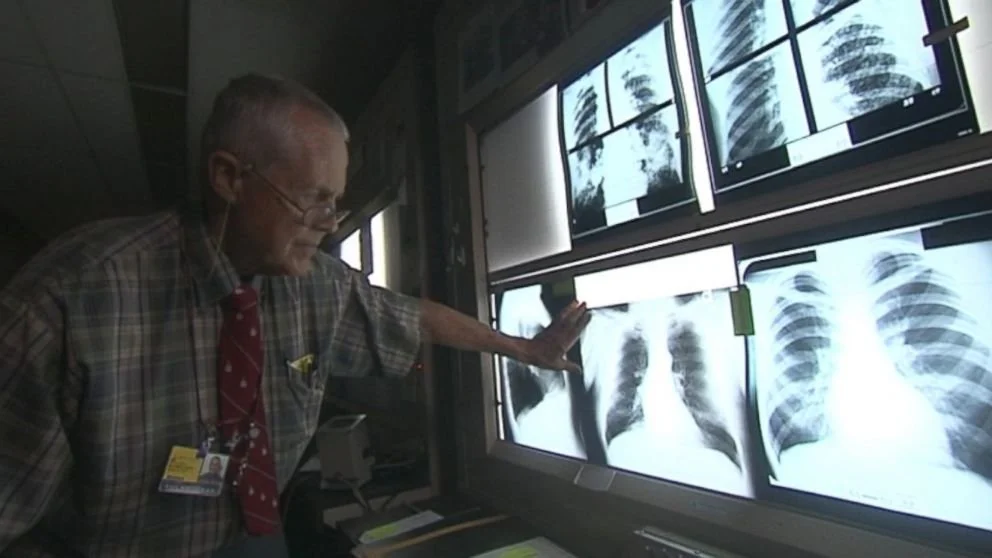
Photo Credit: ABC News

2010
The Upper Big Branch mine disaster remains the deadliest coal mining catastrophe in over four decades. A preventable explosion in Raleigh County, fueled by a build up of coal dust and methane, took the lives of 29 miners at a Massey Energy operation at the Upper Big Branch mine in Montcoal.
Investigators found a direct relationship between the disaster and systematically flawed safety enforcement: mine operators maintained two sets of books to hide hazards, disabled water sprayers designed to suppress dust, and engaged in a conspiracy to falsify coal dust samples that measured exposure to the very substance that caused the explosion. This fraud had devastating impacts following autopsy reports of the deceased. A staggering 71-86% of victims had black lung disease, including some miners who had worked less than five years, at a rate roughly ten times the regional average.
The Upper Big Branch mine disaster exposed how weak federal enforcement and inspector inexperience at MSHA, coupled with a corporate drive to cut safety corners at the expense of profit, allowed Massey’s operators to prioritize production no matter the human cost. For his part, former Massey Energy CEO, Don Blankenship, was convicted of a single misdemeanor count of conspiring to willfully violate mine safety standards. In 2016, Judge Irene Berger sentenced Blankenship to the maximum penalty of one year in prison and a $250,000 fine, making it the first time that a high-profile coal executive was imprisoned for workplace safety violations.

Photo Credit: Roger May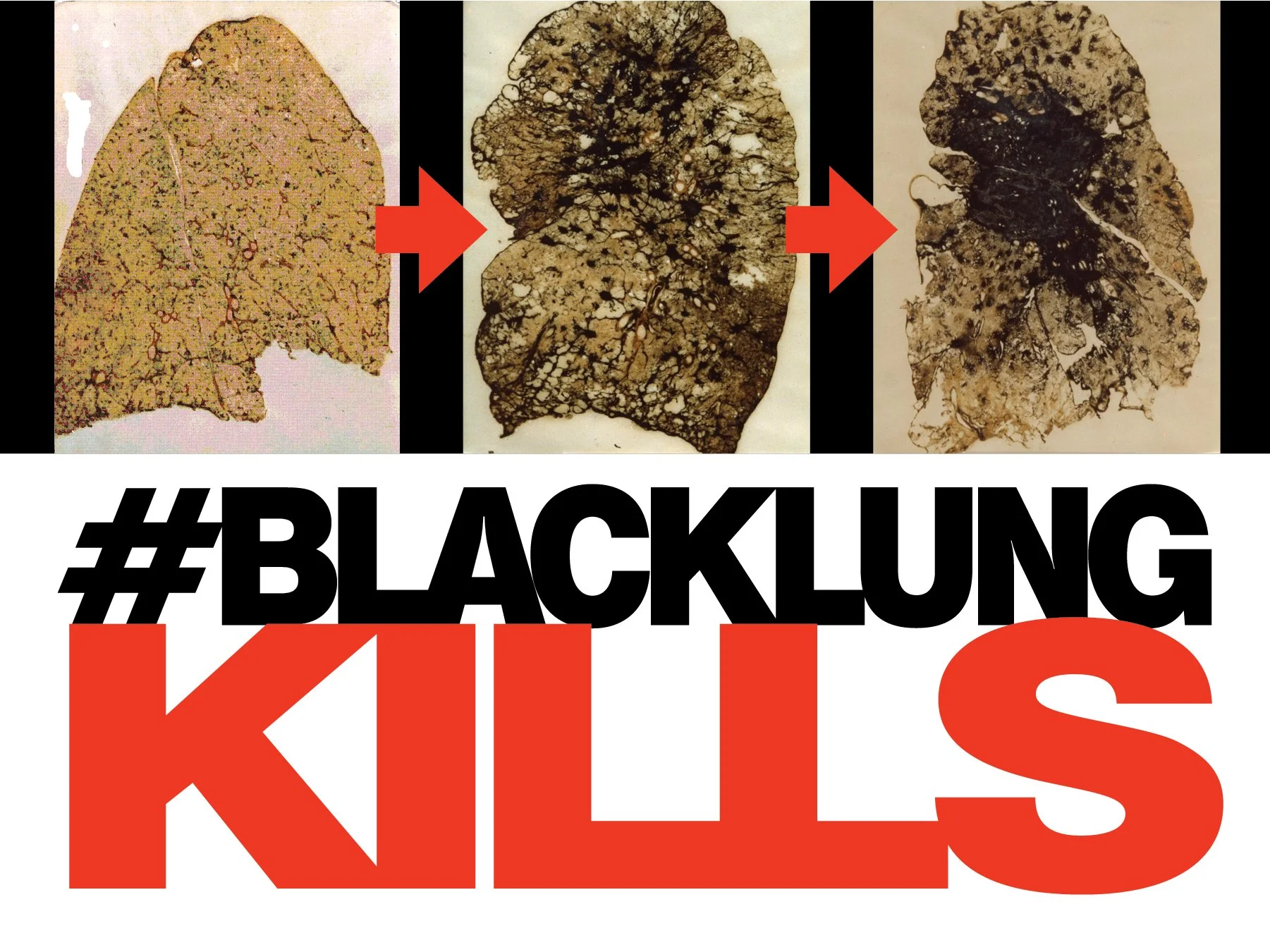

Photo Credit: Pittsburgh Post-Gazette
Photo Credit: WBOY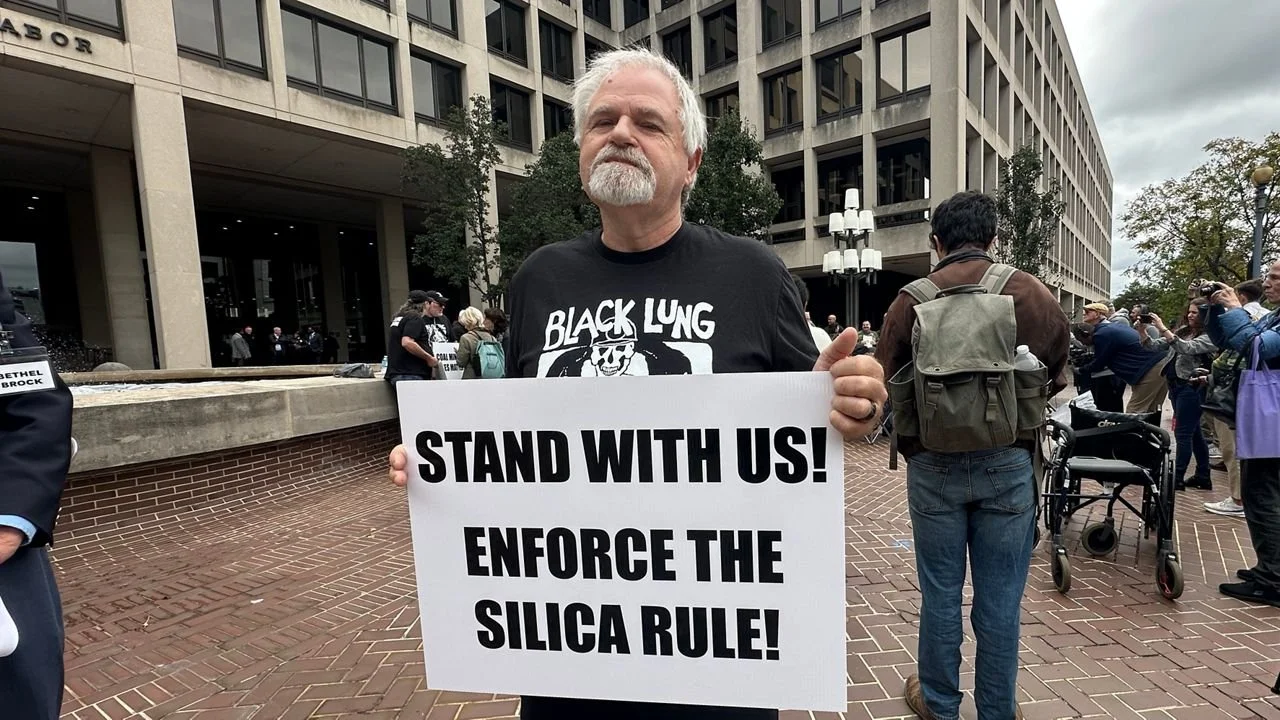
Photo Credit: Spectrum News/Erin Kelly
Photo Credit: NIOSH
Photo Credit: Earl DotterToday
Both of these signature regulatory practices were later rolled back by the second Trump Administration. The silica dust rule faced ongoing litigation from industry associations, and the Trump Administration’s Department of Labor refused to defend the rule in court. At present, the rule is in limbo and miners continue to face risks of preventable occupational health hazards. As for the self-insurance rule, it is currently unclear whether the Department of Labor is enforcing this rule in its current form at all.
A central component of President Trump’s second term initially was cutting government “waste, fraud, and abuse” through the newly-created Department of Government Efficiency (DOGE). In April 2025, DOGE initiated deep cuts to the National Institute for Occupational Safety and Health (NIOSH), firing over 85% of the agency’s staff and shuttering key research centers, which also eliminated key safety programs including those focused on black lung research, medical tracking, and free coal worker health examinations.
DOGE had also initially targeted MSHA field offices for cuts, proposing the termination of 34 MSHA inspector offices across the country, which would have severely limited enforcement capacity. MSHA has already faced understaffing concerns in recent years, losing over a quarter of their total staff over the past decade, raising alarms about the agency’s ability to conduct mine safety inspections. Following community outrage and pushback against both of these proposed cuts, however, the Trump Administration later rescinded these proposals.
However, the Administration has continued to move forward with its anti-regulatory agenda. In 2025, the Department of Labor put forward a series of regulatory rollbacks that would remove the oversight of District Managers, whose role is to help provide additional safety measures for mine training, roof control, and ventilation plans. These new rules would prohibit District Managers from requiring additional safety measures that went beyond existing federal regulations.
While President Trump has issued several Executive Orders prioritizing domestic coal production and use for everything from energy to manufacturing, his anti-labor agenda has continued to harm coal miners by putting them in harm’s way for the sake of company profits.